Table of Contents >> Show >> Hide
- The Day I Heard the Words
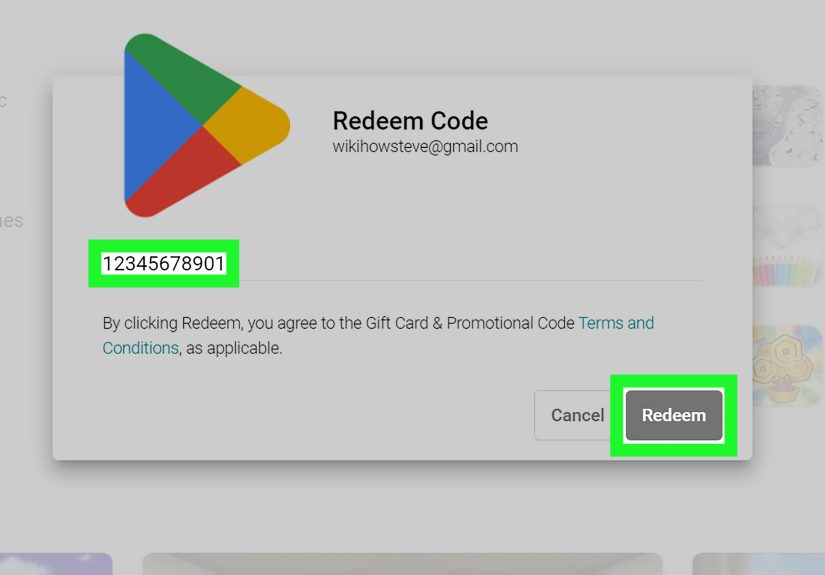
- Step One: Confirm What the Test Means
- Step Two: The Lab Numbers That Suddenly Run Your Group Chat
- Step Three: Starting HIV Treatment (ART) Sooner Than “Someday”
- The Moment I Learned About U=U (And My Shoulders Dropped)
- My “First Week” Survival Kit
- Disclosure: The Question With No One-Size Answer
- HIV Stigma: The Extra Weight Nobody Ordered
- Living With HIV: The “Long Game”
- What About My Partner, My Future, My Everything?
- Common Myths I Had to Kick Out of My Head
- The Part Nobody Sees: Grief, Relief, and the Quiet Middle
- Extra “Diagnosis Diaries” Experiences: The 500-Word Add-On (Because Life Is Never Just One Chapter)
- Conclusion: What I Wish I’d Known on Day One
There are days when your life splits neatly into before and after. Not because you wanted a dramatic plot twistmore like the universe walked into the writers’ room, dropped a folder labeled “HIV,” and said, “Okay, everybody improvise.”
This is a “Diagnosis Diaries” story: part personal narrative, part practical guide, and 100% proof that your brain can hold fear and hope at the same time (even if it tries to file both under “PANIC”). If you’re reading this because you’re newly diagnosedor you love someone who istake a breath. HIV is serious, yes. It’s also treatable. And with today’s care, many people living with HIV go on to live long, full lives with careers, relationships, goals, and the occasional wildly overpriced coffee.
The Day I Heard the Words
I didn’t walk into the clinic expecting a life-changing sentence. I expected something boring: “Drink more water,” “Reduce stress,” “Here’s a pamphlet you’ll never read.” Instead, I got a calm voice, a gentle pause, and the phrase: “Your test came back positive for HIV.”
My first reaction was not inspiring. It was not cinematic. It was mostly my brain sprinting around like a Roomba trapped in a bathroom: bump, panic, spin, repeat.
I had questionssome logical (“What happens next?”) and some deeply unhelpful (“Am I going to be okay?” repeated forty-seven times). The provider did what good providers do: they didn’t rush me, didn’t lecture me, and didn’t make HIV sound like a moral verdict. They talked about next steps.
Step One: Confirm What the Test Means
A lot of people don’t realize that an HIV diagnosis isn’t usually based on a single test and a shrug. Most modern testing follows a sequence designed to be accurate and to catch both established infections and very recent (acute) infection.
The testing “pipeline” in plain English
- Screening test: Often a 4th-generation antigen/antibody test (it can detect HIV antibodies and a viral protein called p24 antigen).
- Follow-up test: If the first test is reactive, labs typically run a test that helps distinguish HIV-1 from HIV-2 antibodies.
- Additional testing (if needed): If results are unclear, a nucleic acid test (NAT) can look for HIV RNAespecially useful for very early infection.
When I heard “positive,” my brain tried to negotiate like it was buying a used car: “Are we sure?” And yesthere was a clear process behind the result. That mattered. It helped me move from spiraling into something more useful: planning.
Step Two: The Lab Numbers That Suddenly Run Your Group Chat
Within the first visits, two terms showed up everywhere: viral load and CD4 count. If HIV is a story, viral load is the number of copies of the virus in your blood, and CD4 cells are part of your immune system’s defense team.
Viral load
Viral load is measured in copies per milliliter (copies/mL). Early on, it can be high. It’s not a “score” of your worth. It’s a medical measurement that helps guide treatment and track progress.
CD4 count
CD4 cells help coordinate immune responses. A “normal” CD4 range varies, but many references describe it roughly in the hundreds to over a thousand. Your CD4 count helps your care team understand how your immune system is doing and whether you need extra protections (like certain vaccines or preventive meds).
Here’s the part nobody tells you: seeing those numbers can feel weirdly personal. Like you got graded on a test you didn’t study for. My provider reframed it: These are starting points, not destiny.
A simple example (not anyone’s real chart)
Imagine a brand-new diagnosis comes with a viral load of 120,000 copies/mL and a CD4 count of 410. That may look scary on paper. But with effective treatment, many people see viral load drop dramaticallyoften to “undetectable”and CD4 can stabilize or improve over time.
Step Three: Starting HIV Treatment (ART) Sooner Than “Someday”
The biggest shift in modern HIV care is this: treatment isn’t something you “wait” for. Current guidelines recommend starting antiretroviral therapy (ART) as soon as possible after diagnosis. Some clinics even offer rapid-start or same-day starts depending on the situation, labs, and access.
When my provider said, “We can start treatment now,” I expected it to feel like defeat. Instead, it felt like someone handed me the steering wheel. Not a magic one. A regular steering wheel. But stillcontrol.
What ART is (and what it isn’t)
- ART is a set of medications that stops HIV from making copies of itself.
- ART is not a cure, but it can control HIV so well that the virus becomes undetectable in blood tests.
- ART protects your health and also reduces the risk of passing HIV to others.
And yesmy brain asked about side effects immediately, because anxiety loves a checklist. Side effects vary by medication and by person. Some people have few or mild side effects; others need adjustments. The point is: you and your clinician have options. HIV treatment today is not what it was decades ago.
The Moment I Learned About U=U (And My Shoulders Dropped)
There are facts that change how you see yourself. For me, one of the biggest was U=U: Undetectable = Untransmittable.
In everyday language: if a person living with HIV takes ART as prescribed and maintains an undetectable viral load, they have zero risk of sexually transmitting HIV to partners. That sentence didn’t erase everything I feltbut it changed the story from “my life is over” to “my life is different, and it’s still mine.”
U=U also did something unexpected: it fought stigma. Not all at once. Not magically. But it gave me science to stand on when shame tried to move in like an unwanted roommate.
My “First Week” Survival Kit
After diagnosis, time gets strange. The minutes crawl, the days blur, and you can somehow spend two hours staring at a wall and still feel busy. Here are the steps that helped me get through the first weekpractical and emotional.
1) Get connected to HIV care quickly
Linking to an HIV-experienced clinic or provider matters. Early care helps you start treatment, get baseline labs, and build a plan that fits your lifenot the other way around.
2) Ask what labs are being ordered (and why)
Common early labs may include viral load, CD4 count, tests for other sexually transmitted infections, hepatitis screening, kidney/liver function tests, and sometimes resistance testing to help choose the best meds.
3) Pick one trusted person (if you can)
You don’t owe anyone your private medical information. But if you have one safe person, telling them can reduce isolation. I chose the friend least likely to panic and most likely to show up with snacks and a plan.
4) Be kind to your nervous system
Eat something. Sleep when you can. Take a walk. Avoid doom-scrolling at 2 a.m. if possible (I say this as someone who absolutely doom-scrolled at 2 a.m.). If your anxiety or depression spikes, it’s not weaknessit’s a human response. If you can access counseling, support groups, or mental health care, they can help.
Disclosure: The Question With No One-Size Answer
“Who do I tell?” might be the hardest question after “Am I okay?”
Disclosure is personal. It can also be complicated by fear of stigma, misunderstanding, or losing relationships. What helped me was separating disclosure into categories:
- Medical disclosure: Your care team needs to know for your health.
- Emotional disclosure: One or two trusted people who support you.
- Relationship disclosure: Depending on your circumstances, you may choose to talk with partners with guidance from a clinician or counselor.
There’s no prize for disclosing before you’re ready. There’s also no rule that you must carry this alone. The “right” pace is the one that keeps you safe and supported.
HIV Stigma: The Extra Weight Nobody Ordered
HIV stigma is real. It shows up as jokes, assumptions, awkward silences, and sometimes discrimination. It can also show up internally as shameespecially right after diagnosis.
I had to unlearn the idea that HIV was a character flaw. It’s a virus. A medical condition. And like many medical conditions, it comes with social baggage that doesn’t belong to the person living with it.
What helped me push back against stigma
- Accurate info: Understanding transmission, treatment, and U=U.
- Community: Even one supportive group or friend changes everything.
- Language: “I’m living with HIV” felt truer than “I am HIV.”
- Boundaries: I don’t owe everyone a debate.
Living With HIV: The “Long Game”
Once the shock settled, real life returnedannoyingly persistent, like laundry. HIV became something I managed, not something that managed me.
Medication adherence (aka, the daily habit that matters)
Taking ART as prescribed is the foundation of treatment. People reach and maintain viral suppression by sticking to their regimen. I made it boring on purpose: same time, same routine, same reminder. If you miss a dose, don’t spiraltalk to your provider about what to do and how to make your plan easier.
Regular monitoring
Your clinic will monitor viral load and sometimes CD4 count on a schedule that changes over timeoften more frequently at the beginning, then less often once you’re stably suppressed.
Whole-person health
HIV care isn’t only about HIV. It’s also about sleep, nutrition, mental health, movement, vaccines, and managing other conditions. The goal isn’t just “survival.” It’s a good life.
What About My Partner, My Future, My Everything?
I wish I could tell you I handled every future-oriented worry gracefully. I did not. I handled them like a human: some days strong, some days messy, some days eating cereal for dinner and calling it “self-care.”
Here’s what’s real and practical:
- Prevention options exist: People without HIV can reduce risk with tools like PrEP; after a possible exposure, PEP can be an emergency option if started quickly (within days).
- U=U changes relationships: If you become and remain undetectable, you can’t sexually transmit HIV.
- Family planning is possible: Many people living with HIV have children safely with modern care and guidance.
Not every conversation is easy. But you’re not walking into them empty-handed. You have treatment, science, and support.
Common Myths I Had to Kick Out of My Head
Myth: “An HIV diagnosis means my life is basically over.”
Reality: With ART and ongoing care, many people live long, full lives. HIV is manageable like many other chronic conditions.
Myth: “I’ll always be a danger to people I love.”
Reality: With sustained viral suppression (undetectable viral load), there is zero risk of sexual transmission (U=U).
Myth: “Everyone will know.”
Reality: Your health information is private. You choose who to tell, when, and how.
The Part Nobody Sees: Grief, Relief, and the Quiet Middle
Diagnosis stories often jump from “shock” to “inspiration” like there’s a fast-forward button. Real life has a long middle chapter. That middle is where I learned to live with uncertainty, build habits, and stop treating every thought like an emergency.
I grieved the version of myself who didn’t have this. I also felt relief that I knewbecause knowing meant treating. I learned that two things can be true at once: HIV changed my life, and my life is still mine.
Extra “Diagnosis Diaries” Experiences: The 500-Word Add-On (Because Life Is Never Just One Chapter)
After the first appointments and the first prescriptions, I expected the hard part to be over. Spoiler: the hard part just got a new outfit. It wasn’t always fear anymoreit was routines, conversations, and the quiet emotional aftershocks that showed up when I least expected them. Like when I was in the grocery store comparing pasta sauces and suddenly thought, “Wow, I’m buying marinara while living with HIV.” It felt surreal, like the universe had layered two realities on top of each other.
The first time I took my HIV medication, I stared at the pill for an embarrassingly long time. I wish I could tell you I had a movie momentsoft light, brave music, meaningful tear. In reality, I was standing in my kitchen in mismatched socks, thinking, “This tiny thing is really about to become part of my daily life.” I took it, drank water, and waited for lightning to strike. It didn’t. The world stayed ordinary, and that was oddly comforting.
Then came the “medical admin” era: portals, lab appointments, pharmacy calls, insurance questions, reminders. If you’ve never had a health condition that comes with a logistics package, it’s a lot. I started treating it like a project (because my brain loves a project when it’s scared). I made a checklist: refill dates, clinic contacts, questions for my next visit, and the one tiny reward I’d give myself after appointmentsusually a fancy iced coffee, because apparently that’s my coping mechanism of choice.
The emotional stuff was sneakier. I’d have a great day, then get hit with a wave of shame like it had my address. In those moments, I practiced a script: “This is stigma talking, not truth.” I learned to name the feeling without obeying it. Some days I needed to talk to someone. Other days I needed to turn off my phone, take a walk, and let my nervous system unclench one muscle at a time.
Disclosure was its own mini-series. I didn’t tell everyone. I told one person firstthe friend who is calm in a crisis and allergic to judgment. When I said, “I have HIV,” they didn’t flinch. They asked what I needed. That moment didn’t fix everything, but it made the world feel less hostile. Later, when I shared with another trusted person, I led with facts: “I’m in care, I’m on treatment, and the goal is an undetectable viral load.” Information became a bridge instead of a barrier.
And thenslowlynormal life returned. Not the old normal. A new normal with reminders on my phone and a deeper respect for my own resilience. I still have hard days. But I also have days that are so ordinary they’re beautiful. HIV is part of my story, yes. It’s not the whole story. It’s a chapter I didn’t ask for, but it’s one I’m learning to write with honesty, humor, and a stubborn commitment to keep living.
Conclusion: What I Wish I’d Known on Day One
If you take anything from my Diagnosis Diaries story, let it be this: an HIV diagnosis is not the end of your life. It’s the start of a new care planand, for many people, a future that is still full of love, work, laughter, and meaningful days.
Get connected to care. Start treatment as soon as you can. Ask questions until the answers make sense. Protect your mental health like it’s part of treatmentbecause it is. And remember: science is on your side, and you do not have to do this alone.