Table of Contents >> Show >> Hide
- What is a subarachnoid hemorrhage (SAH), exactly?
- Symptoms of subarachnoid hemorrhage
- Causes of subarachnoid hemorrhage
- Risk factors: who’s more likely to have an SAH?
- How subarachnoid hemorrhage is diagnosed
- Conditions that can mimic SAH (and why doctors don’t “wait and see”)
- Why speed matters (even though this article isn’t about treatment)
- What to do if you suspect a subarachnoid hemorrhage
- Real-world experiences: what people remember (and what they wish they’d known)
- Conclusion
- SEO Tags
If your body had a “do not ignore” alarm system, a subarachnoid hemorrhage (SAH) would be the
version that kicks the door down and yells your full name. It often shows up as a
thunderclap headachea sudden, severe headache that peaks fast and feels dramatically different
from your usual head pain. This isn’t your brain being “a little stressed.” It’s your brain saying,
“Hey, there’s blood where there shouldn’t be blood.”
Medical note: This article is for education, not diagnosis or treatment advice. If you or someone near you
has a sudden, severe headache (especially with fainting, confusion, stiff neck, vomiting, or seizures),
call emergency services right away.
What is a subarachnoid hemorrhage (SAH), exactly?
A subarachnoid hemorrhage is bleeding into the space between the brain and the thin tissues that cover it.
That space is called the subarachnoid space. Under normal circumstances it contains cerebrospinal fluid (CSF)
and blood vesselsnot free-floating blood from a leak.
SAH is a type of hemorrhagic stroke. And yes, it’s every bit as urgent as it sounds. The blood can irritate
brain tissues, raise pressure inside the skull, and disrupt normal brain function in minutes.
In the U.S., SAH is relatively uncommon compared with other stroke types, but it’s serious enough that emergency
departments treat it as a “move fast and don’t guess” situation.
Symptoms of subarachnoid hemorrhage
SAH symptoms can vary, but there’s a reason clinicians are trained to perk up at certain phrases. SAH often announces
itself in a very specific, very dramatic way.
The classic symptom: “Worst headache of my life”
The most common hallmark symptom is a sudden, severe headache that reaches maximum intensity quickly.
Many people describe it as the worst headache they’ve ever hadand importantly, it feels different from prior
migraines or tension headaches. The speed of onset matters: SAH pain can go from “fine” to “what is happening to my skull?”
in seconds.
Not every thunderclap headache is SAH, but SAH is one of the reasons a thunderclap headache is treated like a medical emergency.
Other common symptoms (your brain’s “plus-one” list)
Along with sudden severe head pain, SAH may come with:
- Nausea and vomiting (sometimes forceful)
- Neck stiffness or neck pain (from irritation of the meninges)
- Light sensitivity (photophobia)
- Vision changes (blurred vision, double vision, or other disturbances)
- Brief loss of consciousness or fainting
- Confusion, trouble concentrating, or unusual sleepiness
- Seizures
- Weakness, numbness, trouble speaking, or other stroke-like symptoms
When symptoms are subtle (and that’s part of the danger)
Sometimes early exam findings can be mild, especially soon after symptom onset. A person might be awake, talking,
and still have a dangerous bleed. That’s why clinicians put so much emphasis on the story: sudden onset, peak intensity,
“different from my usual headache,” and red-flag symptoms.
“Warning” headaches: the leak before the leak
Here’s an unsettling but important concept: some aneurysms can leak a small amount of blood before a major rupture.
This is sometimes described as a sentinel bleed or sentinel headachea sudden, unusual headache days or weeks before
the bigger event. Not everyone gets this warning, and it’s easy to dismiss as “a weird migraine.” But if a severe headache is
sudden, different, or paired with neck stiffness, fainting, vomiting, or confusion, it deserves urgent evaluation even if it improves.
Causes of subarachnoid hemorrhage
SAH can be traumatic (after head injury) or nontraumatic/spontaneous (from a blood vessel problem).
The underlying cause matters because it drives the next diagnostic stepsand the plan to prevent re-bleeding.
1) Ruptured brain aneurysm (the big one in spontaneous SAH)
A brain aneurysm is a weak spot in a blood vessel wall that bulges outward. If it ruptures, blood can spill into the
subarachnoid space. In nontraumatic SAH, aneurysm rupture is the most common cause and is often what clinicians are looking for first.
People often ask: “Wouldn’t I know if I had an aneurysm?” Not always. Many aneurysms don’t cause symptoms until they leak or rupture.
That’s why SAH can feel like it comes out of nowherebecause sometimes, it does.
2) Arteriovenous malformation (AVM) or other vascular abnormalities
An arteriovenous malformation is an abnormal tangle of blood vessels that can rupture and bleed. Other vascular issueslike
certain types of arterial dissectionscan also cause SAH, though they’re less common than aneurysm rupture in spontaneous cases.
3) Head trauma
Trauma is a common cause of SAH overall. A fall, car crash, sports injury, or assault can damage blood vessels and lead to bleeding
in or around the brain. Traumatic SAH can range from mild to severe depending on the injury and the amount of bleeding.
4) Less common causes and contributing factors
SAH can also be associated with (or made more likely by) factors that affect blood vessels or clotting, such as:
- Uncontrolled high blood pressure
- Smoking
- Heavy alcohol use
- Stimulant drugs such as cocaine or methamphetamine
- Bleeding disorders or blood-thinning medications (context-dependentnever stop prescribed meds without medical guidance)
- Inflammatory blood vessel conditions (vasculitis) and certain inherited connective tissue disorders
Risk factors: who’s more likely to have an SAH?
Risk isn’t destiny, but it can explain why doctors ask the questions they do. Some risk factors are modifiable (you can do something about them),
and others aren’t (thanks, genetics).
Risk factors that can often be changed
- High blood pressure (especially if uncontrolled)
- Smoking
- Heavy alcohol use
- Use of stimulant drugs (cocaine/methamphetamine)
Risk factors you can’t change (but should tell your clinician about)
- Older age (risk rises with age for aneurysm-related SAH)
- Family history of brain aneurysm or SAH (first-degree relatives)
- Certain inherited conditions (for example, polycystic kidney disease or connective tissue disorders)
If multiple close relatives have had aneurysms or SAH, clinicians may discuss screening in some circumstances.
How subarachnoid hemorrhage is diagnosed
Diagnosing SAH is a race against timebecause the biggest threat isn’t just the first bleed, it’s complications like re-bleeding or reduced blood flow.
The diagnostic pathway is designed to confirm the bleed, then identify the cause (especially an aneurysm) quickly.
Step 1: A fast, focused evaluation (history + exam)
In the emergency department, clinicians start with the story: When did the headache start? How fast did it peak? Was there a collapse?
Any seizure? Neck stiffness? Recent trauma? They’ll also check vital signs and perform a neurologic examlooking at speech, strength, coordination,
eye movements, and level of alertness.
One detail that matters a lot: the exact time of symptom onset. Imaging accuracy changes over time, and it helps guide next steps.
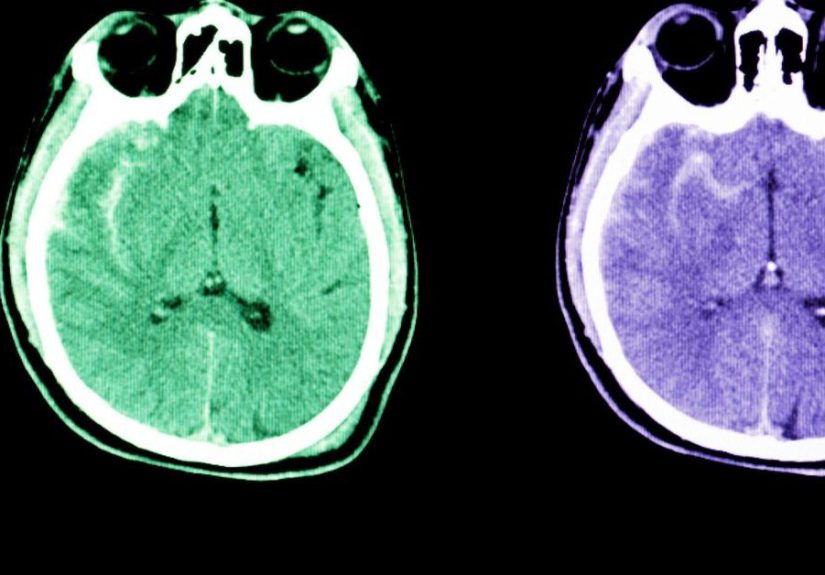
Step 2: Noncontrast CT scan of the head (the usual first test)
The first-line test for suspected SAH is typically a CT scan of the head without contrast. It’s fast, widely available, and very good at detecting
acute bleedingespecially soon after symptoms begin.
If the CT clearly shows blood in the subarachnoid space, clinicians move quickly to identify the source and plan definitive care.
If CT is negative but suspicion remains high, the workup continues (because “not seen yet” is not the same as “not there”).
Step 3: Imaging the blood vessels (CTA, MRA, and angiography)
If SAH is foundor strongly suspecteddoctors often use tests that visualize blood vessels:
- CT angiography (CTA): A contrast-enhanced CT technique that can help detect aneurysms and other vascular problems.
- MR angiography (MRA): An MRI-based method to evaluate blood vessels, sometimes used depending on the clinical situation.
-
Cerebral angiography (catheter angiography): A more invasive test that can provide detailed images and may be used when the cause
is unclear, when initial studies are negative despite strong suspicion, or when planning treatment.
Step 4: Lumbar puncture (spinal tap) when CT doesn’t settle the question
If the CT scan is negative but the clinical suspicion remains strong, clinicians may perform a lumbar puncture to test cerebrospinal fluid (CSF).
The lab looks for evidence of bleeding (including breakdown products that can discolor the fluid, often described as xanthochromia).
The idea is simple: if blood has leaked into the subarachnoid space, signs of it can show up in the CSFeven if the CT is inconclusive.
A lumbar puncture isn’t “fun,” but it can be a crucial test when the stakes are this high.
A quick example of how diagnosis may unfold
Imagine someone who develops a sudden, explosive headache while showering. They don’t hit their head. They feel nauseated, light hurts their eyes, and their
neck feels stiff. In the ER, they get a noncontrast CT head right away. If CT shows bleeding, the team moves to CTA and neurosurgical consultation.
If CT is negative but the presentation screams “thunderclap headache,” further testingoften lumbar puncture and/or vascular imaginghelps rule SAH in or out.
That’s the core philosophy: don’t rely on vibes. Use the right tests in the right order.
Conditions that can mimic SAH (and why doctors don’t “wait and see”)
Sudden severe headache has a wide differential diagnosis. Some causes are benign; others are dangerous. Clinicians move quickly because the symptoms overlap.
Examples that can resemble SAH include:
- Severe migraine (especially first-time migraine or migraine with neurologic symptoms)
- Meningitis (can cause headache, fever, stiff neck, light sensitivity)
- Reversible cerebral vasoconstriction syndrome (RCVS)
- Cervical artery dissection
- Intracerebral hemorrhage or other stroke types
- Pituitary apoplexy
The takeaway is not “panic about every headache.” It’s “respect the red flags,” especially when pain is sudden, severe, and unfamiliar.
Why speed matters (even though this article isn’t about treatment)
Once SAH is suspected, time matters because complications can develop quickly. Depending on cause and severity, SAH can lead to:
- Re-bleeding (especially if an aneurysm is untreated)
- Vasospasm (narrowing of brain blood vessels that can reduce blood flow)
- Hydrocephalus (buildup of fluid in the brain)
- Seizures and other neurologic complications
That’s why emergency evaluation is the rulenot the exceptionwhen SAH is on the list.
What to do if you suspect a subarachnoid hemorrhage
If you think “this could be SAH,” the action plan is refreshingly simple (and deliberately not DIY):
- Call emergency services. Don’t drive yourself if you’re dizzy, confused, or at risk of passing out.
- Note the time symptoms started. That detail is clinically useful.
- Share medication info. Especially blood thinners, aspirin use, or recent drug exposure.
- Don’t minimize it because it improved. Sudden severe headache that’s “different” still needs evaluation.
And if you’re the person with the headache: you are not “being dramatic.” SAH is dramatic. You’re being appropriately concerned.
Real-world experiences: what people remember (and what they wish they’d known)
The following are composite, real-world patterns people commonly describenot specific individuals. SAH is intensely personal, but certain themes show up again and again.
1) “It wasn’t a normal headachemy body made that obvious.”
Many survivors describe the first symptom with the same kind of language: instant, explosive pain. Some compare it to being struck, even when no trauma occurred.
A lot of people say the most frightening part wasn’t just severityit was the speed. One moment they were making coffee, taking a shower,
or bending down to pick something up, and the next they were gripping the counter trying not to vomit.
A common regret is waiting because they didn’t want to “waste the ER’s time.” In hindsight, most say: if a headache is sudden, severe, and unfamiliar,
it’s not the day to practice stoicism.
2) “The symptoms came in a weird bundle.”
People often expect stroke to look like facial droop or one-sided weakness. But SAH can show up as a headache with a strange entourage:
light feels like knives, the neck locks up, nausea hits hard, and thinking gets foggy. A spouse or friend may notice the person
repeating questions, seeming unusually sleepy, or acting “off.”
One practical tip caregivers often share: if someone has a thunderclap headache and then becomes confused or drowsy, don’t debatecall.
Confusion isn’t a personality quirk; it can be a neurologic emergency.
3) “The ER moved fast, and it felt surreal.”
Patients frequently describe the diagnostic process as a blur: quick triage, neurologic checks, a rush to CT, then more tests. That speed can be scary,
but it’s also reassuringbecause it means the team is treating the situation with the urgency it deserves.
For some, the most intimidating part is the possibility of a lumbar puncture. People who’ve been through it often say two things:
(1) it’s not pleasant, but (2) it’s manageable, and it can provide crucial information when imaging is unclear. In other words,
it’s a “short-term discomfort for long-term clarity” trade.
4) “Recovery is a chapter, not a single event.”
Even though this article focuses on symptoms, causes, and diagnosis, lived experience doesn’t end with a scan result. Survivors often describe fatigue,
headaches, sensitivity to stimulation (light, noise, busy environments), and changes in mood or concentrationsometimes for weeks or months.
Caregivers talk about learning a new kind of patience: brain healing doesn’t follow a neat calendar.
Many families also emphasize how valuable it is to keep follow-up appointments and rehabilitation plans, and to ask direct questions:
“What warning signs should send us back to the ER?” “What activity restrictions matter right now?” “What support is available for cognitive or emotional changes?”
The best recoveries tend to look like teamworkpatient, family, and clinicians all pushing in the same direction.
If there’s one shared message across these experiences, it’s this: trust the signal. A sudden, severe headache that feels unlike anything you’ve had before
deserves urgent medical attention. In this particular situation, “better safe than sorry” isn’t a sloganit’s a strategy.






