Table of Contents >> Show >> Hide
- How Breast Cancer Spreads in the First Place
- Lymph Nodes: Usually the First Stop, But Not Always the Final Story
- Bones: The Most Common Place Breast Cancer Likes to Crash the Party
- Liver: A Silent Site Until It Is Not
- Lungs: Sometimes Loud, Sometimes Sneaky
- Brain: Less Common Than Bone, But Never Ignored
- How Doctors Confirm Where Breast Cancer Has Spread
- Treatment After Spread: It Is About Control, Time, and Quality of Life
- What This Means for Patients and Families
- Experiences People Commonly Describe When Breast Cancer Spreads
- Conclusion
- SEO Tags
When people hear that breast cancer can “spread,” the mind tends to sprint straight into the worst-case marathon. That is understandable. It is also exactly why this topic deserves a calm, clear explanation instead of vague internet doom-scrolling at 2 a.m. with a cold cup of coffee.
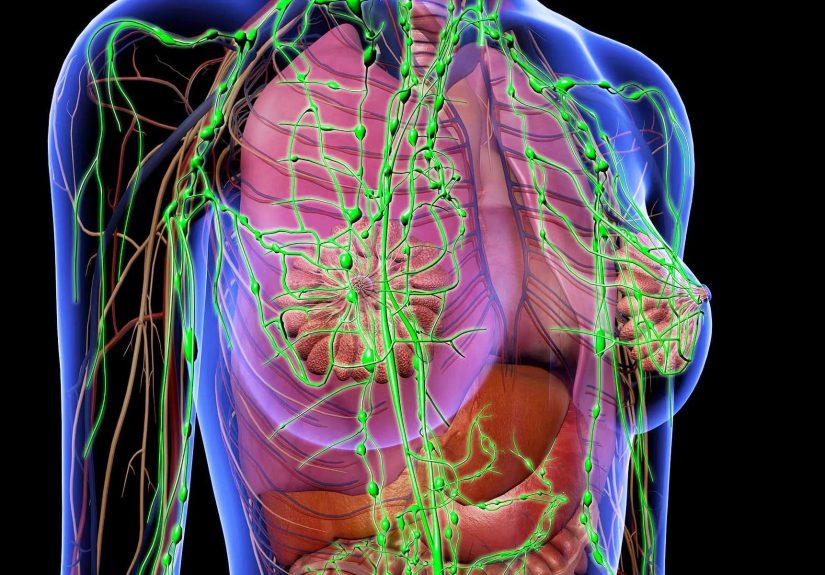
Breast cancer starts in the breast, but cancer cells can sometimes break away and travel through the lymphatic system or bloodstream. When that happens, the disease may show up in nearby lymph nodes first, and in some cases later in distant parts of the body such as the bones, liver, lungs, or brain. These are the places doctors watch most closely because they are among the most common sites of breast cancer metastasis.
Here is the key distinction: spread to nearby lymph nodes is not automatically the same thing as stage IV metastatic breast cancer. Nearby nodes often matter for staging and treatment planning, but distant metastasis means the cancer has moved beyond the breast and regional nodes to other organs or distant lymph nodes. That difference is medically important and emotionally huge.
This guide walks through where breast cancer spreads, what symptoms may appear in each area, how doctors confirm what is happening, and how treatment usually changes once the disease has moved. We will keep the tone human, the information grounded, and the unnecessary drama locked outside where it belongs.
How Breast Cancer Spreads in the First Place
Cancer cells do not politely stay in their assigned seats. Some can invade nearby tissue, enter lymph vessels, or slip into blood vessels. Once they travel, they may settle in another part of the body and start growing there. Even when breast cancer shows up in the bone or liver, it is still breast cancer on a cellular level. That matters because treatment is based on the biology of the original breast cancer, not on the name of the organ where it landed.
Doctors usually pay close attention to three things when spread is suspected: where the cancer is located, whether it is causing symptoms, and what type of breast cancer it is. Hormone receptor-positive disease, HER2-positive disease, and triple-negative breast cancer do not always behave the same way, and they are not treated the same way either.
Lymph Nodes: Usually the First Stop, But Not Always the Final Story
The lymph nodes are often the first place breast cancer goes outside the breast. The most common regional lymph nodes are in the armpit, near the breastbone, and around the collarbone area. Finding cancer in these nearby nodes can affect stage, risk assessment, and treatment recommendations. It can mean the cancer has learned how to travel, but it does not necessarily mean it has spread to distant organs.
What lymph node spread can mean
If cancer is found in nearby lymph nodes, doctors may recommend more systemic treatment because the chance of microscopic spread can be higher. But nearby node involvement still falls into the category of regional disease, not distant metastasis. That is why someone can have lymph node-positive breast cancer and still not have stage IV disease.
Symptoms can include swelling in the underarm, fullness above the collarbone, or tenderness, although many people have no obvious symptoms at all and lymph node involvement is found on imaging or biopsy. Sentinel lymph node biopsy or other node evaluation helps doctors understand how far the disease has traveled locally.
When lymph nodes count as metastatic disease
Distant lymph nodes are a different story. If breast cancer spreads to lymph nodes outside the regional drainage area, doctors may classify that as metastatic breast cancer. This is one reason the phrase “it spread to the lymph nodes” can sound much simpler than it really is. In breast cancer, which lymph nodes are involved matters just as much as whether any are involved at all.
Bones: The Most Common Place Breast Cancer Likes to Crash the Party
Of all the distant sites, bones are among the most common places breast cancer spreads. The spine, ribs, pelvis, and long bones are frequent trouble spots. Why bones? Cancer cells can adapt to the bone environment in a way that helps them survive and grow. It is rude, impressive, and deeply unwelcome.
Common symptoms of bone metastases
Bone metastases often cause symptoms that are hard to ignore, though easy to blame on “sleeping weird” for way too long. Common signs include:
Persistent bone pain, especially in the back, hips, ribs, or legs; pain that gets worse at night; fractures that happen more easily than expected; weakness or numbness if the spine is involved; and trouble walking or moving comfortably.
Not every ache means cancer has spread. Arthritis, strains, and ordinary life can also make the body complain loudly. The difference is that metastatic bone pain tends to persist, worsen, or behave in ways that feel unusual for the person experiencing it.
How doctors treat breast cancer in the bones
Treatment often includes systemic therapy aimed at the cancer overall, plus bone-strengthening medicines such as bisphosphonates or denosumab to reduce fractures and other bone complications. Radiation may help control pain in a specific area. In some cases, surgery or procedures to stabilize weakened bones are needed. Pain management and palliative care are not “extra credit” here; they are part of good cancer care.
Liver: A Silent Site Until It Is Not
The liver is another common destination for metastatic breast cancer. The tricky part is that liver metastases may not cause obvious symptoms at first. Some people learn about them because of abnormal imaging or blood tests rather than a dramatic physical warning sign.
Possible symptoms of liver metastases
When symptoms do show up, they may include fatigue, loss of appetite, nausea, unintentional weight loss, discomfort or pain in the upper right side of the abdomen, bloating, a feeling of fullness, or jaundice if liver function becomes impaired. Because these symptoms can overlap with treatment side effects, stomach bugs, stress, or simply having the world’s most annoying week, doctors often rely on scans and lab work to clarify what is going on.
How treatment changes when the liver is involved
Most treatment is still systemic, which means medicine that circulates through the body. Depending on tumor biology, that may include hormone therapy, targeted therapy, chemotherapy, HER2-directed therapy, or immunotherapy in selected cases. If a liver lesion is causing a specific problem, local treatments may sometimes be considered, but the larger strategy usually focuses on controlling the disease throughout the body, not just in one organ.
Lungs: Sometimes Loud, Sometimes Sneaky
Breast cancer can also spread to the lungs or the lining around the lungs. Some people have no symptoms at first, while others notice changes that feel a lot like ordinary respiratory issues. Unfortunately, a “maybe it is allergies” theory only works until it does not.
Common symptoms of lung metastases
Typical symptoms can include a persistent cough, shortness of breath, wheezing, chest discomfort, and reduced exercise tolerance. In some cases, fluid can build up around the lungs, causing a pleural effusion. That can make breathing feel harder and may require drainage if it becomes significant.
Because cough and breathlessness have many possible causes, doctors usually look at the whole picture: symptoms, exam findings, imaging results, treatment history, and whether fluid or lesions are visible on scans.
How lung metastases are managed
Again, systemic therapy is usually the backbone. If breathing symptoms are prominent, treatment may also include procedures to manage fluid, oxygen support in selected cases, or local radiation for problem areas. The goal is not just to treat scans. It is to help the person breathe, move, sleep, and function more comfortably.
Brain: Less Common Than Bone, But Never Ignored
Brain metastases are not the most common first site of spread, but they are a major concern because they can affect speech, movement, vision, memory, and safety. Some breast cancer subtypes, especially HER2-positive and triple-negative disease, have a higher tendency to spread to the brain than others.
Symptoms that can point to brain metastases
Symptoms may include persistent or worsening headaches, dizziness, vision changes, weakness, numbness, trouble with balance, confusion, behavior changes, nausea, vomiting, or seizures. These symptoms deserve prompt medical attention because they can progress quickly and may require urgent imaging.
Treatment options for brain metastases
Treatment may include radiation therapy, surgery in selected cases, steroids to reduce swelling, and systemic therapies that can work in the brain for certain tumor types. The plan depends on how many lesions are present, where they are located, how large they are, and what treatments the person has already had.
One important point: brain involvement does not erase the rest of the treatment plan. Doctors still look at the whole cancer picture, not just the MRI headline that ruined everybody’s afternoon.
How Doctors Confirm Where Breast Cancer Has Spread
Symptoms matter, but symptoms alone do not diagnose metastasis. Doctors often use imaging such as CT, PET, MRI, or bone scans, along with blood work and sometimes biopsy. A biopsy can confirm that a suspicious spot is truly metastatic breast cancer and may also reveal whether the biology has changed. That matters because hormone receptors and HER2 status can sometimes differ from the original tumor, which can alter treatment choices.
For someone newly diagnosed with early-stage breast cancer and no signs suggesting distant disease, extensive metastatic testing is not always necessary. But if symptoms, lab abnormalities, or higher-stage features raise concern, doctors may investigate further.
Treatment After Spread: It Is About Control, Time, and Quality of Life
Once breast cancer has spread beyond the breast and regional nodes, treatment usually shifts from a cure-focused local strategy to a long-term disease-control strategy. That sounds heavy because it is heavy. But it is not the same as “there is nothing to do.” In fact, there is often a great deal to do.
Systemic treatments used in metastatic breast cancer
Depending on the tumor’s biology, treatment may include hormone therapy, targeted therapy, chemotherapy, HER2-targeted drugs, antibody-drug conjugates, or immunotherapy in selected patients. Many people move through several lines of treatment over time, switching when a therapy stops working or side effects become too difficult.
Local treatments still matter
Radiation, surgery, or other local procedures can still play an important role when a specific metastasis is causing pain, threatening function, or creating urgent problems. For example, a painful bone lesion may respond well to radiation, and a brain lesion may need focused treatment even while the rest of the disease is managed systemically.
Palliative care is not giving up
Palliative care deserves a standing ovation and much better public relations. It focuses on symptom relief, emotional support, family support, and quality of life at any stage of serious illness. It can be added early, alongside cancer treatment, and often helps people feel better and function better.
What This Means for Patients and Families
If you are trying to understand spread, the biggest takeaway is this: breast cancer does not spread randomly in a way doctors completely ignore, but it also does not follow a perfect map. Nearby lymph nodes are often the first checkpoint. Bones, liver, lungs, and brain are the most common distant sites. Symptoms vary by location, and treatment depends heavily on the subtype of breast cancer and the person’s overall condition.
That means two people with “metastatic breast cancer” may have very different experiences, very different scan results, and very different treatment plans. The phrase is one diagnosis, but not one story.
Experiences People Commonly Describe When Breast Cancer Spreads
Beyond the scans and medical terms, there is the lived experience, which rarely fits neatly into a textbook chapter. Many people describe metastatic breast cancer as a strange mix of routine and uncertainty. One day you are discussing school pickup, grocery lists, or a work deadline. The next day you are learning the difference between a PET scan and an MRI like that was definitely on your life bingo card.
When the cancer spreads to lymph nodes, some people feel shocked because they assumed lymph node involvement automatically meant the worst. Others feel confused when doctors explain that nearby lymph node spread is serious but not the same as distant metastasis. That gray area can be emotionally exhausting. It is not just a medical distinction. It changes how people think about prognosis, treatment, and the future.
People with bone metastases often talk about how pain can creep into everyday life. Sitting in a chair too long hurts. Rolling over in bed hurts. Reaching for a coffee mug suddenly feels like an activity that should come with training. The emotional challenge is that pain is not just painful; it is interruptive. It steals sleep, shortens patience, and makes normal life feel oddly unfamiliar.
When the liver is involved, the experience may be less about one dramatic symptom and more about a gradual sense that something feels off. Fatigue becomes heavier. Appetite goes missing. Food may taste ordinary at best and offensive at worst. Some people say the hardest part is that these changes can be invisible to others, so they look “fine” while feeling anything but fine.
Lung metastases can make the world feel smaller. Walking across a room, climbing stairs, or speaking in full sentences may suddenly require more effort. That loss of ease can be frightening. Breathing is one of those things people usually never think about until breathing starts thinking about them first.
Brain metastases can be especially unsettling because they may affect not only the body but also memory, mood, language, or confidence. A headache is one thing. A headache plus balance changes or vision changes is something else entirely. Patients and families often describe this stage as emotionally intense because symptoms can interfere with independence in very personal ways.
Across all metastatic sites, one shared experience is “scanxiety,” the stress that builds before tests and follow-up visits. Even people who appear calm on the outside may be running a full internal disaster rehearsal. Many also describe the importance of a care team that explains things clearly, responds to symptoms quickly, and treats quality of life as a real medical priority rather than a side note.
Support matters here more than most people realize. Counseling, support groups, palliative care, physical therapy, pain specialists, social workers, and practical help from friends or family can all make a real difference. People living with metastatic breast cancer often say they want honesty, options, and the freedom to keep living their lives in meaningful ways. Not perfectly. Not magically. Just meaningfully.
And that may be the most important experience-related truth of all: even when breast cancer spreads, life does not become only about cancer. It becomes more medically complicated, yes. But people still make plans, celebrate milestones, laugh at bad hospital coffee, worry about regular bills, and text loved ones about completely non-medical nonsense. Disease may take up more space, but it does not automatically get the whole house.
Conclusion
Breast cancer most often spreads first to nearby lymph nodes and, when it becomes metastatic, commonly to the bones, liver, lungs, and brain. Each site can bring different symptoms, different risks, and different treatment decisions. The big picture is not just where the cancer traveled, but how it behaves, what subtype it is, and how treatment can control the disease while protecting quality of life.
If there is one message worth keeping, it is this: “spread” is not one-size-fits-all language. Nearby lymph nodes are not the same as distant organs. Bone pain is not the same as liver dysfunction. A cough is not the same as a seizure. Precision matters. Compassion matters too. And when both show up together, patients are far better served.